This article appears in the July/August issue of Surgical Products.
A 36-year-old male was brought to the Cook County Trauma Unit after sustaining multiple trans-abdominal gunshot wounds to the abdomen and right groin in October of 2009. The initial operation was damage control with primary repairs to the right colon. The patient developed a massive SIRS response and remained non-closeable for several weeks. He returned to the operating room every three days for negative pressure dressing (VAC) changes and abdominal washouts. Subsequent operations included a right hemi colectomy with primary iliocolic anastomosis for breakdown of his prior repairs. He remained with an open abdomen in the trauma ICU.

During his multiple take backs to the operating room, he developed an anastomotic leak at the iliocolic anastomosis. This was repaired primarily on two occasions, but the leak recurred. At that time, the abdomen was deemed non-closeable due to domain loss. Abdominal integrity was restored using a 20×30 centimeter Surgimend 3.0 mesh placed as a bridge. The mesh was sutured within the retro rectus space laterally and bridged a span of 13cm mid-wound fascial gap by 35 cm long. The technique used to implant the mesh was a modified Reeve Stoopa method where by the retro rectus space was opened and a pocket the length of the wound was created. The mesh was seated into this pocket behind the rectus muscle and in front of the posterior rectus sheath. Using several counter incisions in the anterior abdominal skin, the mesh was secured in place with a #1 pds suture. The abdominal skin was then closed over the bridging mesh and drains. Approximately one week later, recurrence of the anastomotic leak at the superior apex forced the superior portion of the skin to be opened and a small ostomy was constructed through the mesh. This leak was controlled using a negative pressure dressing and eventually was bagged with an ostomy bag.
After a several-month protracted and complicated hospital course, the patient successfully convalesced and was discharged home tolerating a general diet, ambulating, and able to accomplish his activities of daily living after a brief stay in an inpatient rehabilitation facility.
The patient was seen multiple times in follow up. His instructions upon discharge were to exercise daily and continue weight loss (his initial pre-op weight was well over 300 pounds and his discharge weight was 240 pounds). The patient was instructed to refrain from smoking and continue to lose weight. He was followed by the trauma nutrition service monthly and successfully lost 60 pounds over the next year.
During his follow-up, he demonstrated only mild eventration of his bridge mesh graft. He was able to do a limited sit-up but was unable to work. He remained with a controlled ostomy/fistula at the superior apex of his midline scar. This was controlled with an ostomy bag.
In follow up consultation, as his condition continued to optimize, he was scheduled for surgery to take down his fistula.
On November 18, 2011, approximately two years post his initial injury and operation, the patient was taken back to the operating room for excision of his fistula, removal of his bridge graft and subsequent abdominal reconstruction using Trans-Abdominal Wall Traction (TAWT).
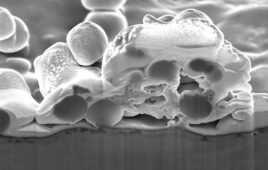
At this time the patient was taken to the operating room, and after extensive adhesion lysis his abdomen was successfully entered. The entire bridge graft, with the exception of the areas adhered to the fascia, was removed, explanted, and sent for histology. The iliocolic anastomosis/fistula was taken down, resected, and re-anastomosed. A large non-closable ventral defect measuring 22 centimeters wide by 35 centimeters long remained. Due to prolonged operation, need for resuscitation, and extensive anticipated fluid shifts, the risk of abdominal compartment syndrome remained high and thus TAWT insertion was delayed. Instead, a negative pressure wound therapy device was placed along with an internal plastic adhesion barrier and the patient was taken back to the Trauma ICU to be resuscitated. He was placed into the Trauma Open Abdomen Protocol (OAP), which delays TAWT placement until near dry weight and physiologic steady state are achieved. The patient returned to the operating room on November 21 for washout and replacement of the negative pressure wound therapy device. TAWT was again delayed at that time, as the patient was not at his near dry weight.
On November 23, he was returned to the OR for wash out and evaluation for TAWT. At this time, TAWT was inserted. The initial mid-wound fascial gap was reduced from 22 centimeters to eight centimeters wide, with the length remaining at 35 centimeters long. He was subsequently tightened, according to the OAP, a series of three times, eventually reducing the defect to less than one centimeter wide. At that time, the abdomen was deemed closeable. The TAWT device was removed and the abdomen was primary closed at the level of the anterior rectus sheath using #1 PDS suture. The closure was re-enforced using a 10×15 centimeter Surgimend 3.0 mesh placed as an underlay using a modified parachute method placing counter incisions along the lateral rectus sheath. The skin was closed using staples.
The patient continued to receive glutamine and tube feeds by dobb hoff tube post operatively. He began a regular diet upon return of flatus. He was discharged to home post op day 10 from his second admission. At that time he was tolerating a regular diet, ambulating freely, and able to accomplish all his activities of daily living. An abdominal binder was placed upon discharge and he continues to wear it.
The patient has been seen frequently in follow-up. He has had no post operative complications and demonstrates no evidence of midline hernia recurrence. He is back to work as a laborer.