Osteoporosis is an epidemic afflicting millions of aging individuals worldwide. One in three women and one in five men over the age of 50 will experience a broken bone due to the low bone mass associated with this insidious disease. By 2020, one in two Americans over 50 will be at risk for osteoporotic fractures. More than 700,000 people annually suffer from vertebral compression fractures (VCF), making them more common than hip and wrist fractures combined. 1,2
The challenge of treating VCFs
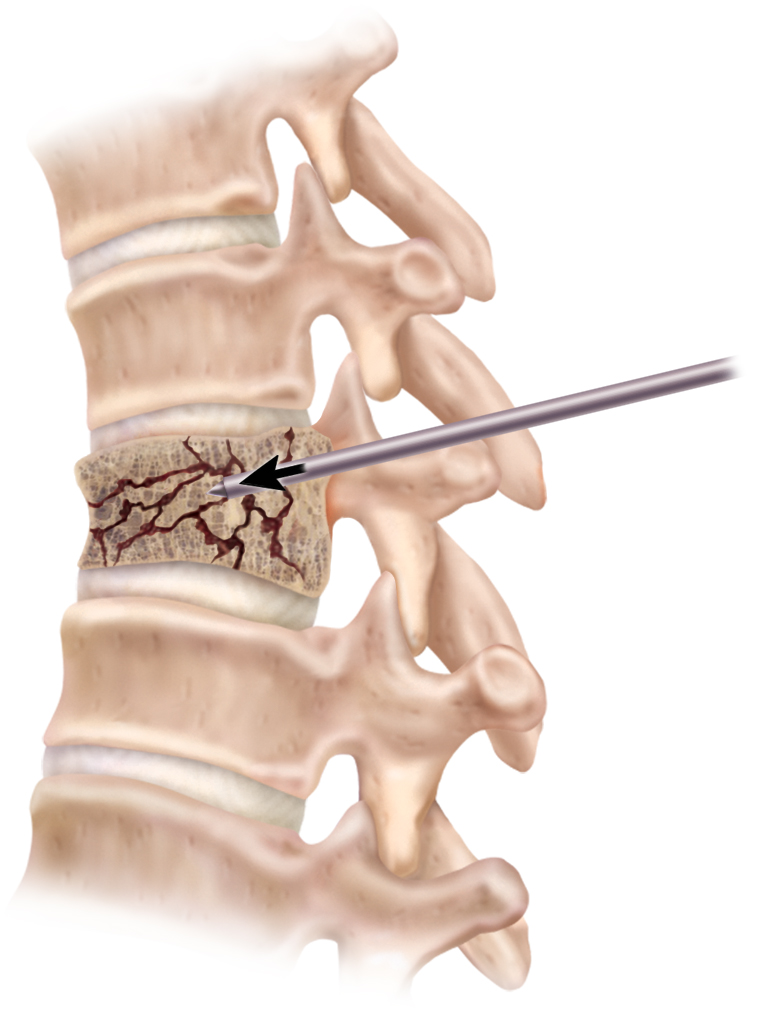
VCFs are just what they sound like: fractures of spinal vertebrae under compressive load. Most commonly, VCFs occur in patients with osteoporosis or some forms of cancer. Such pathologic VCFs can occur from common everyday actions like sneezing or reaching. VCFs can vary in severity and morphology, but the vertebra typically collapses more in the front, resulting in a wedge shape which causes a kyphotic (hunch-back) deformity, thus negatively affecting posture and pulmonary function. This type of fracture is particularly debilitating, with a broken back leading to a downward spiral of complications, including chronic back pain, reduced height, balance and mobility, decreased quality of life, and increasedmortality rates. 2
Broken bones are typically treated using orthopedic principles of fracture management. The aim is to reduce (i.e., restore a normal anatomical shape) and fix (i.e., immobilize the fracture to allow healing) the fracture. This can be easily accomplished via manipulation and casting for long bones of the arm or leg. Vertebral bones pose a greater challenge due to the anatomy, such as the irregular shape and size of the vertebra and their proximity to the spinal cord.
The elegance of balloon kyphoplasty
Balloon kyphoplasty* (BKP) is an innova tive interventional procedure for treating VCFs. Performed with the patient under conscious sedation (awake but sedated), a small skin incision is made and a cannula is inserted through a pedicle into the vertebral body under fluoroscopic guidance. A manual drill creates space for a balloon to be inserted into the vertebral body, with two radio-opaque marker bands indicating the balloon location within the vertebra. The balloon is inflated with radio-opaque contrast liquid under fluoroscopic visualization to monitor the inflation pattern within the vertebra. The omnidirectional balloon expansion lifts the endplates and restores the anatomical shape of the vertebra. The balloon is then deflated and removed, leaving behind a void. This void is fi lled with bone cement, which acts as an internal cast to stabilize the fracture.
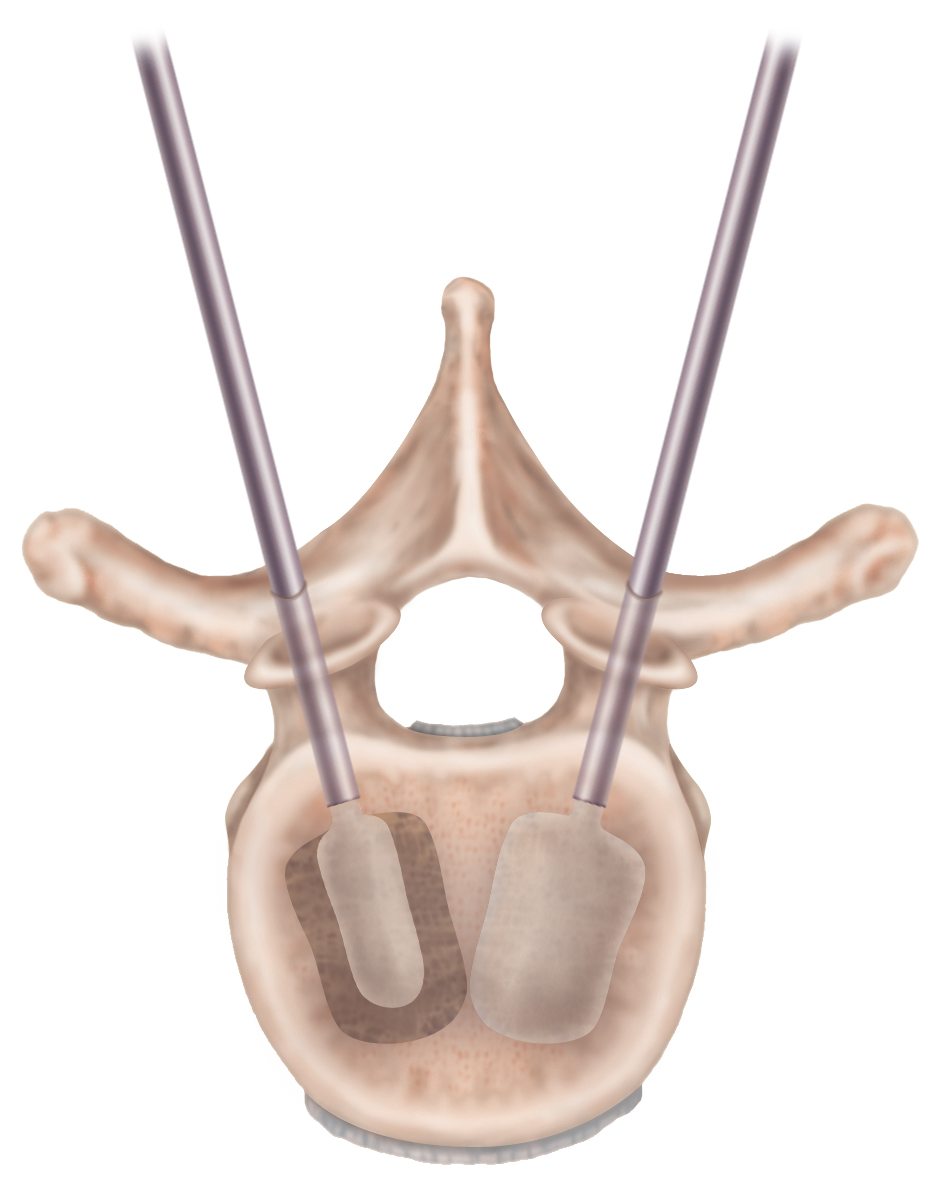
Access to the fractured vertebral body is made with small diameter stainless steel tools (i.e., a solid rod stylet and a cannulated working
channel). A cannula is placed through each pedicle for bilateral access. Inflatable bone tamps (IBTs) are placed through the cannulas and inflated to reduce the fracture. Once the desired reductionis achieved, the IBTs are defl ated and removed, leaving behind a void. The resulting void is fi lled with bone cement, which acts as an internal cast to stabilize the fracture. BKP is typically performed on an out-patient basis, and patients can go home
Access to the fractured vertebral body is made with small diameter stainless steel tools (i.e., a solid rod stylet and a cannulated working channel). A cannula is placed through each pedicle for bilateral access.
the same day. Inflatable bone tamp (IBT) technology comprises forming a balloon from extruded plastic tubing and mounting this onto the end of a stiffer plastic shaft. A Y-adapter on the proximal end allows a removable stylet for column strength and a port for connecting an inflation syringe. The peanut-shaped balloon is inflated into a sausage shape, providing a flattened surface for maximizing surface area to lift endplates. The balloon represents an elegant solution because it is able to be inserted through a narrow diameter cannula and then inflated to a larger diameter to open up space around it. Inflatable balloon catheters are used in other anatomical locations, such as to open up blocked arteries, but bone represents a particularly challenging environment. The ability to engineer a balloon capable of being inflated within bone is a unique mechanical engineering challenge. Such challenges include the trabecular bone within a vertebra being of heterogeneous density, resulting in pockets of harder bone adjacent to sections of softer bone. This may be due to uneven fracture healing during the time before the patient undergoes BKP. Harder pockets are more difficult to reduce than softer bone, and can present sharp points that induce stress points in a flexible material. However, a flexible material has the advantage of distributing stress more evenly along the vertebral endplate, thereby reducing the chance for violating the endplate as compared to a rigid material that may have a high stress concentration.
Infl atable bone tamps (IBTs) are placed through the cannulas and infl ated to reduce the fracture. Once the desired reduction is achieved, the IBTs are defl ated and removed, leaving behind a void.
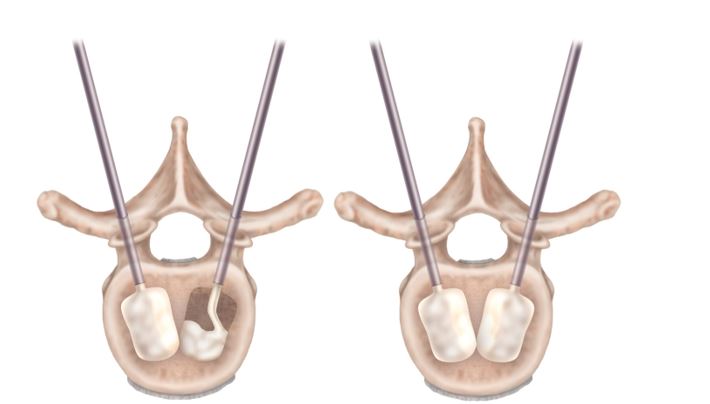
The resulting void is filled with bone cement, which acts as an internal cast to stabilize the fracture.
Reduce and fix the fracture
Since balloons tend to inflate into the path of least resistance, they thus may form “balloon animals” inside a fractured vertebra, assuming an irregular shape rather than the desired inflation pattern. Careful material selection and processing helps to produce less compliant balloons with greater control,
or a tendency to inflate to a pre-determined shape, similar to how mylar balloons inflate into shapes like stars or hearts. Detailed engineering allows the IBT to be rated to a maximum inflation pressure as high as 700 psi without rupturing, providing high power in generating a large force potential for lifting the vertebral endplates and reducing the fracture. Achieving this balloon shape and pressure during inflation helps to maintain the fracture reduction during introduction of polymethylmethacrylate (PMMA) bone cement into the newly-formed cavity. Our balloon material is known to rupture when in contact with PMMA. Thus, a cement resistance technique has been developed to increase the amount of possible contact time and thus prolong the fracture reduction. By offering physicians access to the latest balloon technology, we are now able to offer the ability to control inflation pattern and the power to lift vertebral endplates, along with the ability to deliver bone cement while maintaining reduction. Based on the largest clinical study comparing BKP and non-surgical management (Boonen et al., JBMR 2011), patients experienced reduced pain, improved function, deformity correction, and most importantly, improved quality of life.3
1. National Osteoporosis Foundation Website. www.nof.org
2. Brunton S, Carmichael B, Gold D et al. Vertebral compression fractures in primary care: recommendations from a consensus panel. J Fam Pract. 2005 Sep;54(9):781-8.
3. Boonen S, Van Meirhaeghe J, Bastian L, et al. Balloon kyphoplasty for the treatment of acute vertebral compression fractures: 2-year
results from a randomized trial. J Bone Miner Res. 2011;26(7):1627-1637. *`Balloon Kyphoplasty incorporates technology developed by Gary K. Michelson, M.D.
Disclaimer from Medtronic: BKP is a minimally invasive procedure for the treatment of pathological fractures of the vertebral body due to osteoporosis, cancer, or benign lesion. Keep in mind that results of this procedure may vary, and all treatment and outcome results are specific to the individual patient. Results may vary. A prescription is required. The complication rate for balloon kyphoplasty has been demonstrated to be low. There are risks associated with the procedure, including serious complications, and though rare, some of which may be fatal. These include, but are not limited to heart attack, cardiac arrest (heart stops beating), stroke, and embolism (blood, fat or cement that migrates to the lungs, heart, or brain). Other complications include infection and leakage of bone cement into the muscle and tissue. Cement leakage into the blood vessels may result in damage to the blood vessels, lungs, heart, and/or brain. Cement leakage into the area surrounding the spinal cord may result in nerve injury that can, in rare instances, cause paralysis. Please consult your physician for a complete list of indications, contraindications, benefits, and risks. Only you and your physician can determine whether this procedure is right for you. For more information, visit www.spine-facts.com.
Balloon Kyphoplasty incorporates technology developed by Gary K. Michelson, M.D.


