Surgeons want to quickly treat people who need unique patient-specific implants. Point-of-care generation of these devices will meet this need.
Mark Wehde, Mayo Clinic

Mechanical designer Robbie Highet (left) consults with mechanical engineer Joel Kuhlmann on the design of a custom implant. (Image courtesy of the Mayo Clinic)
Engineers have long understood the value of reverse engineering as a technique for extracting knowledge from an existing design. There are many reasons to do so, but for the purposes of this article the best reason would be to develop an understanding of a legacy system, often to replace obsolete parts in order to return something to its previous level of functionality.
Point-of-care additive manufacturing of implants is primarily an extension of this technique applied to patients. While standard orthopedic implants are appropriate for many procedures in which the implant size and shape can be standardized, such as hip implants, there is a significant number of use cases where that simply isn’t possible.
When custom implants are needed
One of the most common uses of a custom implant is in craniofacial repair, which require a custom implant that matches the patient’s anatomy. A patient might need craniofacial repair because of broken bones, a deformity or a tumor removal that also required the removal of a significant portion of the bony structure. These implants can widely differ due to the variance in the sizes and shapes of tumors or the damage that requires bone to be carefully pieced back together.
Titanium’s biocompatibility, strength and durability make it one of the most commonly used materials for these types of implants. A typical implant for a mandibular reconstruction uses bone harvested from the patient’s fibula. An engineering team then uses CT scans of the patient’s anatomy to develop a custom metal brace or splint to align the implant to the patient’s jaw.

Figure 1 (Image courtesy of the Mayo Clinic)
Once the computer-generated model is created, it can be printed and fit-tested using a traditional polymer print of the patient’s jaw, as shown in Figure 1. This method is superior to the traditional method of bending and cutting to shape during the surgical procedure. Patient anatomy can be hard to match, and there are always concerns about sterility when the implant is handled and manipulated.
The computer-generated model is much more accurate and precise. It allows the implant to be created, inspected, sterilized and packaged before surgery. Particularly challenging anatomy can be addressed before the patient’s arrival, allowing the entire surgery to proceed much more smoothly.

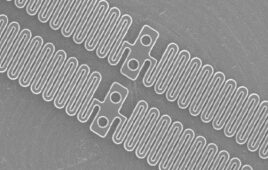
Figure 2 (Image courtesy of the Mayo Clinic)
Figure 2 shows the metal brace printed using support material on an EOS M290 titanium printer. Unlike traditional polymer printers with easily removable support material, the support material for titanium printers is also titanium. Once the powder is vacuumed off, the implant must be separated from the support material using traditional machining techniques.
The value of on-site design and production
Custom implants are commercially available. However, Mayo Clinic’s 14-plus years of experience developing polymer-printed anatomical models for pre-surgical planning has demonstrated the value of having the biomedical engineers and technologists working hand-in-hand with the surgeons and radiologists.
Locating a facility within the surgical suite allows the surgeons to drop-in between cases to consult on the implants being developed. This allows for rapid development of patient specific implants that can be used almost immediately.
Significant work must be done before the printing of custom implants is a more widespread reality. Point-of-care manufacturing of custom implants will not only create better results for patients, but will yield much greater patient satisfaction. This will allow for better patient care and provide extensive training and educational opportunities for both clinical and engineering staff.
Mark Wehde is chair of the Mayo Clinic Division of Engineering, a member of the South Dakota State University Electrical Engineering Industry Advisory Board, and on the board of governors for the IEEE Technology and Engineering Management Society. Mark is also a juror for the Medical Design Excellence Awards, an affiliate for the University of Minnesota Medical Industry Leadership Institute, and a member of the FDA Center for Devices and Radiological Health Network of Digital Health Experts.
The opinions expressed in this blog post are the author’s only and do not necessarily reflect those of Medical Design and Outsourcing or its employees.