 David Novotny, Senior Vice President Medical Device and Diagnostics, Novella Clinical
David Novotny, Senior Vice President Medical Device and Diagnostics, Novella Clinical
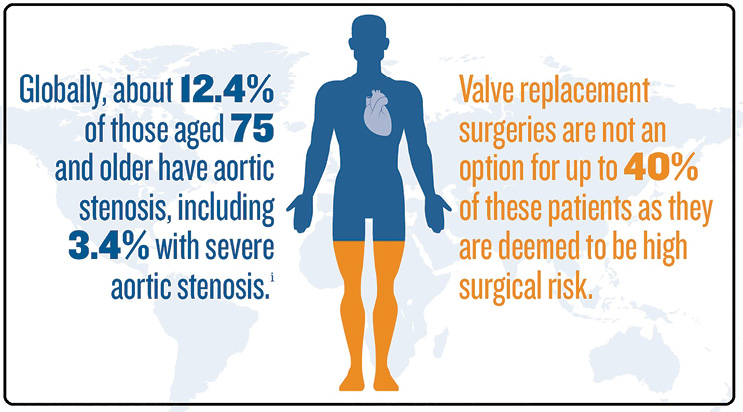
The standard of care for moderate and high-risk patients with severe aortic stenosis – transcatheter aortic valve replacement (TAVR) – may soon be matched by transcatheter replacement of a mitral valve, a market potentially four times the size of TAVR. Developments for TMVR and upcoming clinical trials should give hope to the millions of people unable to undergo even minimally invasive mitral valve repair.
Significant mitral valve regurgitation (leaking) occurs in 2 to 3% of the general population, affecting more than 176 million people globally, including 7.8 million in the United States. However, only about 70,000 mitral repair or replacement surgeries occur in the U.S. each year due to the procedure’s high risk.
It seemed the solution was on a fast track to approval, but that is not the case. TAVR procedures have become the standard of care for prolonging lives and improving life quality. However, applying that same technology to mitral valves (TMVR), which work just millimeters away from aortic valves, is likely years away from the U.S. market.
Until then, here are three headlines I expect to read over the next four years, as well as a glimpse at the road that may lead us there.
Future headline #1: Delays in TMVR device development continue
How we get there: Let innovation take its course.
Since 2000, at least 30 devices in this space have gone through benchmark and animal testing, and have entered or are ready to start clinical trials. The setbacks these trials experienced have disappointed stakeholders, but cynics only compare the results with the rapid success of TAVR. The mitral valve has a much more complex structure than the aortic valve. A replacement must anchor a perfect seal in a space that is not a neat circle as is the aortic valve. Instead, it is a much more chaotic space between two physiologically different, beating chambers of the heart. By realistic measures, innovations abound in the TMVR device space. Almost all the devices in clinical trials use different design strategies.
Ahead of us we expect to see a few more hurdles as device makers explore new ways to address the variability in valve structure from patient to patient, particularly because the device must serve a larger, more mixed patient population than TAVR technology.
Future headline #2: Wave of TMVR device companies announce PMA submissions
How we get there: Secure long-term results with long-term planning
At least eight clinical trials are using TMVR devices as of fall 2016. That makes a decent mix of products that could hit the mark in terms of design. But most of these trials are early-stage. Some trials have seen suboptimal short-term mortality rates, while others have stalled from slow enrollment.
Studies will advance as longer-term outcomes are reported which means device makers and CROs should pay close attention to how they screen participants for long-term implications. In particular, trials should aim at enrolling patients who are on optimal and stable medical regimens. The Mitral Valve Academic Research Consortium recommends sponsors pre-define the criteria for medication dosing stability before randomization to remove any impact it might have on possible effects of the device and clinical outcomes.
Future headline #3: TMVR devices: Durable and safe in at-risk populations
How we get there: Preempt ambiguous results with clearly defined endpoints
The Research Consortium has identified 10 clinical endpoints for all TMVR trials:
- Mortality
- Hospitalization
- Neurological events
- Myocardial infarction
- Access and vascular complications
- Bleeding complications
- Acute kidney injury
- Arrhythmias and conduction system disturbances
- Device and procedural success and specific device-related technical failure issues and complications as well as secondary endpoints involving quality-of-life measures
- Functional performance and echocardiographic assessments including residual mitral valve regurgitation (MR) and perivalvular leaks
The complicating factor is that MR can stem from many more pathologies than aortic valve stenosis, and can lead to more comorbidities, which blurs the endpoint data. To that end, the Research Consortium instructs TMVR trials to differentiate and stratify patients between primary and secondary (functional) MR.
The success of TAVR has created an opportunity for advancing transcatheter approaches for mitral regurgitation patients. Although the future of TMVR is more complex, we will be scanning headlines for good news and waiting for the data demonstrating that TMVR devices safely reduce mitral regurgitation, prolong patients’ survival, and improve quality of life. A white paper, “Innovations in Heart Valve Technology,” is available here: http://tinyurl.com/Innovation-in-heart
[Want to stay more on top of MDO content? Subscribe to our weekly e-newsletter.]