Adding disinfection with UVC LEDs is a viable alternative to chemicals, according to Crystal IS. Here are three examples of how they can make a difference.
Rajul Randive, Crystal IS

[Image courtesy of Crystal IS]
In 2017, the Centers for Disease Control & Prevention (CDC) reported significant progress in many areas commonly associated with hospital acquired infections (HAIs). However, on any given day about one in 25 people who visit a healthcare facility in the U.S. will still contract an HAI.
Infection reduction depends on combating pathogens that are becoming increasingly resistant to chemical disinfection methods. Adding disinfection with UVC LEDs is a viable alternative to chemicals because it disrupts the DNA of harmful microorganisms and destroys their ability to reproduce, thereby eliminating the spread of MRSA, C. diff. and many other pathogens that have no known natural defense mechanism to UVC energy exposure. Although there are many ways to integrate UV disinfection with LEDs throughout the hospital, the following cases offer the most opportunity for near term impact on the rate of HAIs.
1. Preventing C. diff Infections on high-touch surfaces
Clostridium difficile (C. diff.), one of the most-reported HAIs, causes nearly 500,000 illnesses per year. It’s a remarkably resilient pathogen that’s easily transported on high-contact devices including mobile phones, stethoscopes, workstations and diagnostic tools. These devices are usually cleaned with chemicals such as isopropyl alcohol – but alcohol wipes do not kill C. diff. UVC LEDs provide a method for a quantifiable and trackable UVC disinfection dose via handheld or countertop devices to combat the superbug. In addition, integration directly into portable workstations and diagnostic equipment allows surface disinfection as hospital staff transition between patient rooms.
2. Quantifiable hub disinfection for CLABSI reduction
The CDC reported a 50% reduction in central-line-associated blood stream infections (CLABSI) between 2008 and 2014, but recent improvements have been less dramatic. Disinfecting the hub of a central line is a manual process that relies on friction and time. It takes up to 60 seconds when executed properly and there is no way to verify compliance. A handheld LED device attached to an infuser could be aimed at the hub and within seconds deliver a UVC dose capable of a 4-log reduction of common pathogens like MRSA. The result is that a consistent disinfection dose is applied to a common site of pathogen transport in far less time.
3. Preventing ventilator-associated pneumonia
UVC LEDs can also be used to address ventilator associated pneumonia (VAP). Though it occurs in only 1% to 2% percent of patients using mechanical ventilators, VAP mortality rates are greater than 50%. Focused UVC energy from a LED-enabled device could disinfect complex passageways, in-vitro components and even nebulizer equipment in-situ without heating the target surfaces.
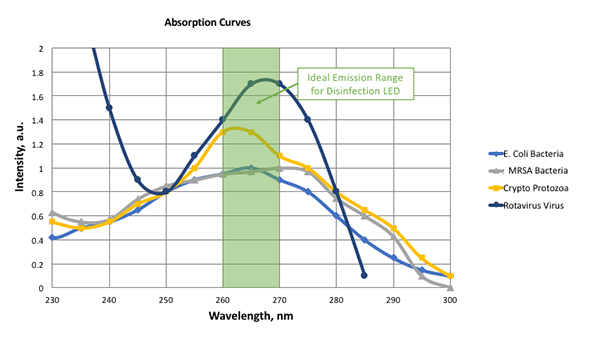
[Graph courtesy of Crystal IS]
Considerations for selecting a UVC LED
When working with LEDs, there are number of parameters designers need to consider. The primary factor centers around the desired log reduction, or disinfection rate, of the specific target microbe in the application. This defines the UV dosage required which designers need to achieve while balancing the other variables like UV intensity, disinfection time and uniformity of the UV radiation pattern in the design.
Each target microbe has a unique radiation absorption, or “fingerprint,” meaning they absorb UV photons differently at different wavelengths based on their cell structure. The accompanying graph shows the absorption spectra for a few common microbes found in healthcare settings.
The absorption curves show that there is a significant drop in microbe sensitivity at wavelengths shorter than 255 nm and greater than 275 nm. To ensure maximum disinfection performance, design engineers select a UVC LED that offers the greatest overlap of the target microbes absorption spectra, most typically with a peak in the 260 nm–270 nm range.
Once an LED is selected with the optimal peak emission, designers then consider the amount of UV intensity required over a given time to achieve the disinfection target – this is known as dosage. To achieve a high dosage in a short amount of time to address CLABSI, the application would require high intensity. For applications that have more time for disinfection like high-touch surfaces or VAP applications, lower intensity LEDs can be used.
Healthcare providers, medical device OEMs and disinfection equipment manufacturers have every reason to embrace smaller, portable devices that employ solid-state technology like UVC LEDs. Doing so will significantly bolster what’s projected to be a long and difficult fight against the spread of infectious diseases and the ongoing emergence of chemical resistant super bugs.
Rajul Randive is director of application development at Crystal IS (Green Island, N.Y.), responsible for designing, building and testing various prototype applications that use Crystal IS UVC LEDs.





