
Mark Pizzuto [Image from Crystal IS]
According to the Centers for Disease Control & Prevention (CDC), one in every 25 hospital patients in the U.S. will contract a hospital-acquired infection (HAI) during their visit. Often expensive and sometimes fatal, HAIs are adding billions to the country’s already bourgeoning healthcare costs.
For decades, hospitals and other healthcare facilities have employed ultraviolet germicidal irradiation systems (more recently referred to as germicidal UV or GUV), equipped with low-pressure mercury vapor lamps as an added layer of disinfection for a variety of applications ranging from operating rooms to the air circulating in the building’s ductwork.
Although effective, these lamps are inherently cumbersome and too fragile to address the growing need for smaller, lightweight, portable disinfection devices. As an alternative medical device manufacturers are turning to deep-ultraviolet (UVC) light-emitting diodes (LEDs), which offer a substantially smaller footprint and directional UV light in the optimal 250 nm to 280 nm wavelength range for disinfection.
Whether part of a large, comprehensive system or a portable device, UVC LEDs represent a major upgrade: They deliver UVC light in optimal wavelength(s) for improved disinfection; have a much smaller footprint; and consume far less energy due to their instant on/off capability. However, it should be noted that LEDs are not simple plug-and-play replacements for existing applications using mercury lamps. For maximum design flexibility and disinfection efficacy, it’s important to understand the target microbe’s spectral response curve, UV dosage requirement, distance to the source and residence time available within the system.
Examining UV susceptibility by microbe
When developing a UVC disinfection device, the two most critical parameters for calculating dosage are the intensity of the light source (expressed as mW/cm²) and the exposure or residence time/duration the microbe is exposed to UVC energy. By understanding the dosage requirements, an LED sterilization device can be created to match even the smallest disinfection target.
Crystal IS recently contracted with a third-party microbiological testing facility to measure the level of UVC LED disinfection achieved on common target microbes. The log reduction (the number of microbes eliminated from a surface by disinfection) for each microbe was measured after UVC exposures of 30, 60 and 120 seconds at a distance of 2 in. from the light source (Figure 1). The data shows that after 120 seconds the log reduction varied from just over 1 log reduction to up to a 6-log reduction for MRSA.
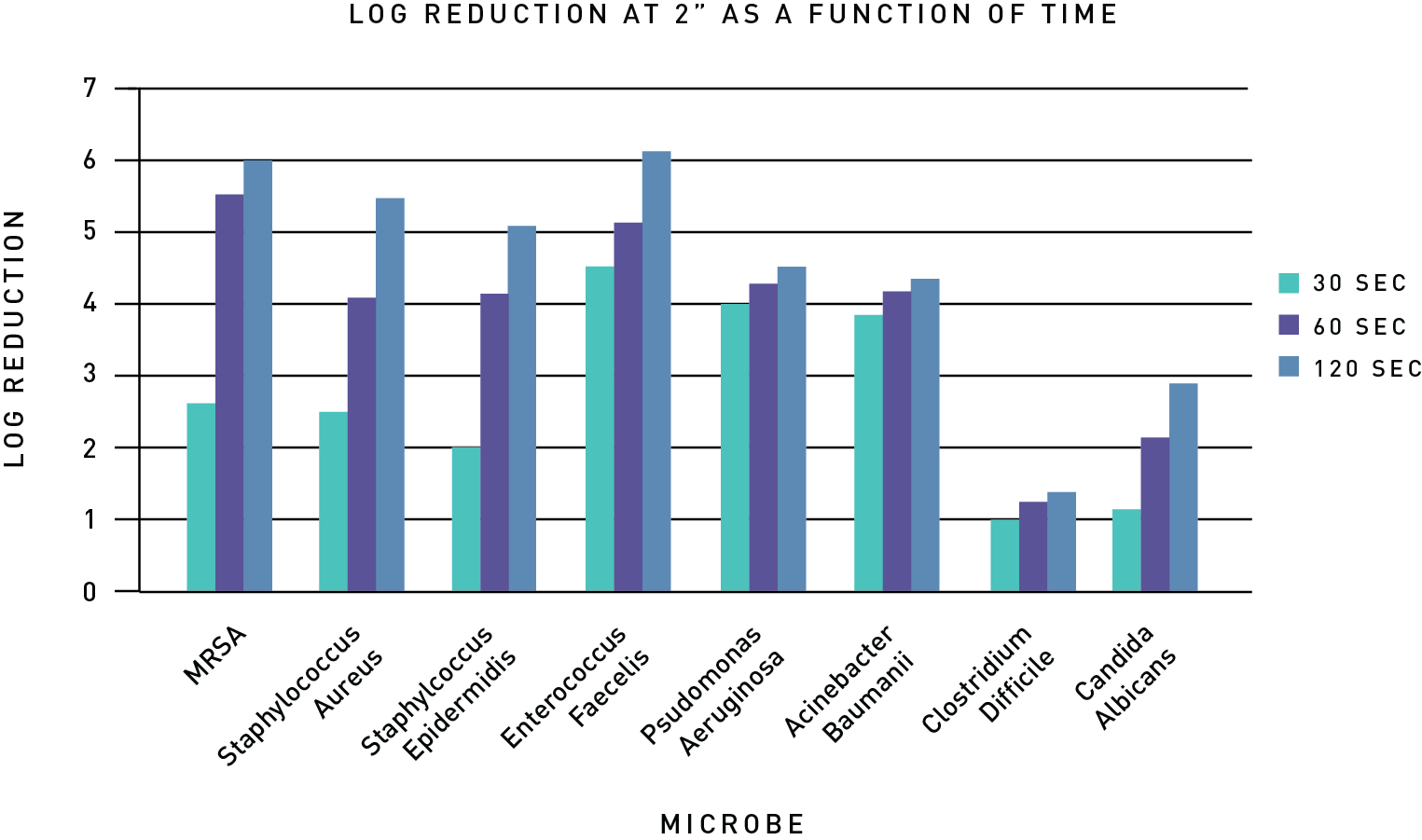
Figure 1: Log reduction as a function of time for various microbes at 2 in. distance.
If the distance between the light source and the surface is increased while holding the time and UVC power constant, the log reduction will be lower. However, the decrease is not linear and can be unpredictable, suggesting dosage calculations should be validated through microbiology studies to confirm the actual results.
Achieving uniform disinfection with design flexibility
Complete exposure of a surface, regardless of shape, will allow for optimal dosage. The compact footprint of UVC LEDs enables better disinfection of small or irregular objects. By leveraging the much smaller, solid-state LED footprint, new disinfection devices can be created to emulate the shape of the intended target.
Understanding UV disinfection is line-of-sight irradiation; Figures 2 and 3 illustrate how the LEDs can be configured to deliver uniform light dispersion across two very different surfaces – a cylindrical vial and a small workstation.

Figure 2: Arrangement of LEDs for disinfection of vials (A), the optical modeling of the irradiation of the vial (B), and the irradiation pattern at the bottom of the vial (C).
In Figure 2, a cylindrical vial requires a dosage of 5mJ/cm2. First, the designer considers the power and time required to achieve that dosage at the furthest point from the LED array – the base of the vial, which is 81 mm from the light source. While the irradiation will be higher near the top of the vial, delivering the minimum dosage to the base ensures the entire vial is disinfected. Therefore, this arrangement will achieve the required dosage after 10 seconds.
Figure 3 illustrates the disinfection of a workspace surface 100mm wide (4 in.), requiring a dosage of 12mJ/cm2. The LEDs are in a 100mm-wide strip of 4 UVC LEDs approximately 25mm above the surface. To achieve a uniform dispersion with the 100° viewing angle, the LEDs are placed 25 mm apart. The target dosage can be achieved by irradiating the surface for 60 seconds.

Figure 3: Arrangement for surface disinfecting bar that can move along the axis (A) and radiation pattern from the LED on to a surface in stationary mode (B).
Being able to arrange LEDs to accommodate a specific surface enables medical device engineers to create a whole new generation of reliable devices that deliver uniform and highly efficient UV disinfection. As a result, manufacturers can develop innovative and, when necessary, customized solutions for specific high-contact surfaces.
Summary
According to the CDC, microorganisms and viruses have developed numerous resistance mechanisms that enable them to evade the effects of antimicrobials, antivirals and chemical treatment.
With medical care being now administered in a range of settings – including the home – the need for portable disinfection equipment to protect patients and clinicians from drug-resistant pathogens and life-threatening infections has never been greater.
In fact, considering the professional/non-professional cross section of potential users – the FDA’s usability standards for new product development suggest that ease-of-use will be a key ingredient in future medical device designs.
As such, all indications are that UVC LEDs will play a major role in the development of next generation disinfection devices.
(See the best minds in medtech live at DeviceTalks West, Dec. 11–12 in Orange County, Calif.)
